 |
| This is a photo of Eli when he turned one. It's a good shot of his scars and his MicKey button. Photo courtesy of Reflections by Mindy. |
People are always curious about his feeding tube. Some of the most popular questions are about how it works, what exactly do we use it for, how often we change it, does it hurt him, and how long will he have it? This post is an explanation of why Eli has the tube, how it works, and answers to the previous questions. So here goes!
Does it hurt him?
No, the tube doesn't hurt him. It was a surgery to put it in and, yes, he was in pain postoperatively, but now it's just part of him. He has been playing with it more these days and I know he's going to pull it out on his own sometime, but for now he just touches it. I don't mind his curiosity, it's part of his body and he needs to be comfortable with it.
 |
| This was the first picture taken of him after having surgery for his feeding tube placement. If you follow the green wire it runs into the disc that was part of the feeding tube. It's difficult to see but there's a white tube coming off that disc. The disc & the tube make up the outer portion of his newly placed feeding tube. The wires were to monitor his heart rate & rhythm and respirations. 02/14/2011 |
Why does he have it?
One of the things that led us to seek help prior to his diagnosis was that he wasn't nursing as much as he had been. We are a family who likes to eat so we knew something was wrong! After his first heart surgery, the only thing he would allow in his mouth was a pacifier...and only a certain brand at that. The fact is Eli needed nutrition, he wasn't eating and we had to have a way to get milk into our baby. Initially, he had an NG (N = nasal G= gastro, meaning a tube inserted into his nose and fed down into his stomach). It had to be taped to his face, immediately made him look different, had to be changed weekly or more often, had to be checked for proper placement prior to each use which was multiple times day and night, and could easily be dislodged or pulled out by Eli or Zachary (Z was only 3 when Eli had the NG). Then he started having bloody stools. It was about two weeks after we got home from his first heart surgery and we didn't know if he had GI problems or if we had scratched him when we changed the tube. Further testing revealed he had a milk protein intolerance. While he was in the hospital for that, our cardiologist made a push to get the feeding tube surgically placed. Bryan and I were on the fence about the permanent need but agreed that if we were going to do it, this was the time. The GI doctor wanted to do an EGD (a tube down the throat into the stomach to allow the doctor to see the tissues and take samples for biopsy) and colonoscopy (a tube up the rectum and through the intestines for the same reason) and Eli would need to be put out for those. Since he was going to be under anyway it was the perfect time to place the feeding tube. Our decision was made and we have not had one regret since.
How long will he have it?
I don't know. Some parents whose little ones have feeding tubes are very anxious to get them removed and I understand that. It's not a natural part of your baby. It's a visual reminder that something is wrong with your perfect child. Bryan and I weren't thrilled about getting it in the first place, but once we did we quickly realized how much better it is for Eli. We are not in any hurry to get rid of it. He had stopped requiring tube feedings for several months, but is now needing them again. We're so glad we have that access. As long as the hole stays healthy and the surrounding skin doesn't have any breakdown, we're much more content to have the button and not use it a lot than to be rid of it and need it again.
How did they get it in there to begin with?
It was a surgery and it took two doctors. One was our pediatric GI (gastrointestinal) Dr. Maisel and the other was a pediatric general surgeon Dr. Kokoska. Dr. Maisel had the scope in Eli's stomach for the EGD and found the spot for the G-tube from the inside. By the way, at this point it was called a G-tube meaning gastric tube (gastric = stomach). Dr. Kokoska found Dr. Maisel's spot from the outside and made the incision where Dr. Maisel wanted it. It took two of them because the internal organs in babies that small are very close together and they didn't want to inadvertently puncture other organs. Remember, Eli was under 10lbs at this point. At first it was a long tube about 18 inches in length that led to a disc on the outer part of his belly. The pictures below were taken throughout the procedure and show what it looked like on the inside. He kept this tube for almost two months. Have you ever had your ears pierced and had to keep the original piercing studs in for a few weeks before you were allowed to change them? This is the same concept. Once the hole had time to form a tract, he was put under anesthetic once again so that tube could be removed and his new button put in place. It's called a MicKey button and it's what you'll see in later pictures.
 |
| Photos given to us by the doctors who placed his G-tube. Image 2 notes point out his liver and his stomach. Image 4 notes say "stomach" and "pulling PEG tube". Doesn't he have the cutest little internal organs ever?!?! |
How often do we change it?
Monthly or more often if necessary.
What necessitates a change?
-if the tube is pulled out
-if the tube is blocked and we can't get anything to flow through
-if it's getting visibly dirty/gunky.
Who changes it? Where is it changed?
We change it. We do it at home, usually on the changing table in his room. We carry an extra kit in our van in case we have to while we're out sometime. Bryan and I have always done it together but one person could do it alone. It's easier with two because one can occupy Eli while the other gets it done. The whole process takes less than 5 minutes. Some people have asked if we're allowed to change it because I'm a nurse while other families would have their doctor do it or go to the hospital. No, I'm not Eli's nurse, I'm his mommy. We were taught, as his parents, to do this regardless of our occupations.
Shouldn't this be done in a sterile environment?
The initial surgery was done in a sterile operating room, but since then it's been what's called a "clean" procedure. When it was converted from the larger tube they placed during surgery to his current MicKey style button, that was in a procedure room, not a sterile OR. Each of his new kits is in sterile packaging. We wash our hands and keep the whole process as clean as possible by laying him on a clean blanket, only touching what we have to, and keeping his hands away. Stomach contents are not sterile like other organs. He probably gets more germs from what he puts into his mouth than from us changing his button.
Here's what you've all been waiting for. Here's how we change it and use his MicKey button.
 |
| This is the kit for his new MicKey button. |
 |
| We use good ole KY jelly (or the generic!) on the stem of the button to make insertion easier for him. So if you see me buying it by the case at WalMart, that's why. Yeah, that's why. |
 |
| This is the new button. I'm holding it upside down so you can see the stem that will be inserted into the hole in his belly. The bottom part is actually the button that stays on the outside of his body. There's a "balloon" that goes around the stem and gets inflated with water. That's how it stays anchored inside his belly. We have to test the balloon prior to inserting the button to make sure it's intact. |
 |
| Here's the balloon after I filled it with 6ml of water (slightly over a teaspoon). It doesn't look like it here, but this balloon only goes around the stem, not over the end of it. The end is open so that his medicines and formula can flow through. The balloon is like an inner tube around the stem. The narrow area between the inflated balloon and the bottom of the button is 1 centimeter in length. That's the part that goes along the tract that was formed between the outside and inside of Eli's belly. When we reorder his buttons from the pharmacy we specify a 14 French (has to do with the diameter of the tube) 1 cm. As he grows, the diameter shouldn't change but the depth probably will. |
 |
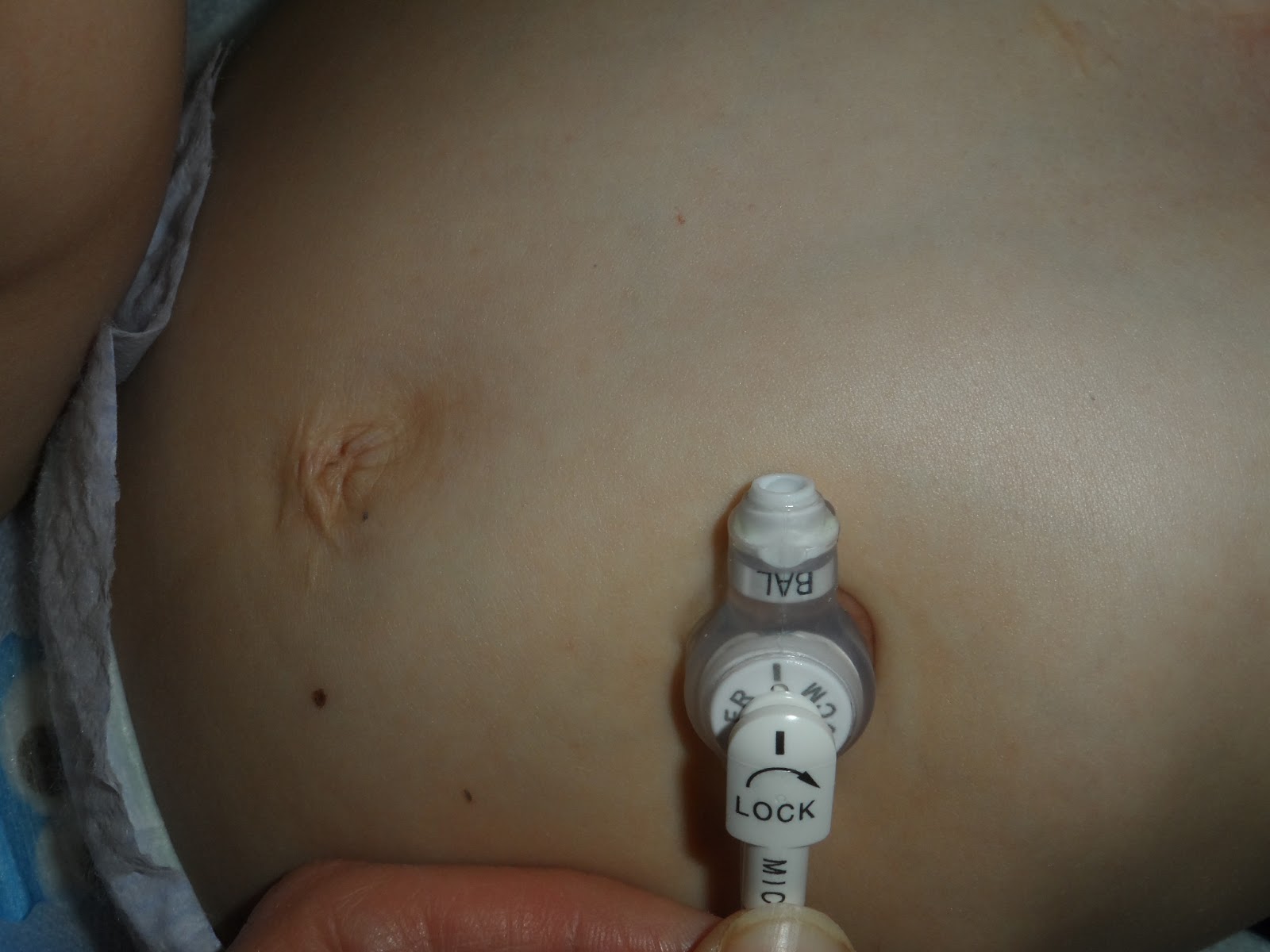
| Here's a different syringe attached to the button that's currently in place. We have to deflate this to take it out. It could get pulled out with the balloon inflated but that would hurt and possibly cause some tearing around his hole. It could happen, but so far he hasn't pulled it out on his own. We hope he doesn't, but I bet if he does it once he won't do it again. Once we pull the water out of the balloon the whole button just lifts out. |
 |
| A view of the hole after his button is removed. We clean it every day and apply some ointment around it to help keep the skin in good shape, but when we change his button it's a good opportunity to really clean it. We just have to be fast because this is a direct opening into his stomach. Yes, gravity is a factor here. If he rolls to his left side very much we may get some stomach contents to pour out. Don't worry, I didn't take any pictures of that. Incidentally we make sure to keep food & drink away from him for about an hour before we do this! Let's just say we've learned the hard way :) |
 |
| Another view of his button hole. |
 |
| The new button is in place, the balloon filled, and the syringe removed. The new button stem just slides into the hole, we inject the water to fill the balloon and remove the syringe. He's done! |
 |
| Here's the tube we use to access his button. The end of the tube has a little piece of plastic that sticks up. That aligns with the notched area on the face of his button. |
 |
| The black line on the access tube shows where the notch is. Line that up with the line on the button indicating the place for the notch and.... |
 |
| ...turn clockwise just shy of a full turn. That locks the tube into place and makes it "become one" with the button. To remove it, simply reverse the process by turning the tube counterclockwise until the black lines line up. Then just take out the tube and replace the doo-hickey rubber piece over the button opening so that other stuff doesn't get in there. The button has a one-way valve inside so things shouldn't leak out once they're in, but if it's been used for a while we may get some occasional leakage (another indicator that it's time to change the button). |
 |
| This is the tube we took out. As you can see, it gets dirty, gross and gunky. |
 |
| It's very hard to see, but there's a small pinpoint opening at the bottom of this stem. That's what all his meds, formula and water pass through into his stomach. Even if we aren't using his tube for medicines or feedings we still have to flush it with water two times a day just to make sure that tiny opening doesn't get clogged. |
 |
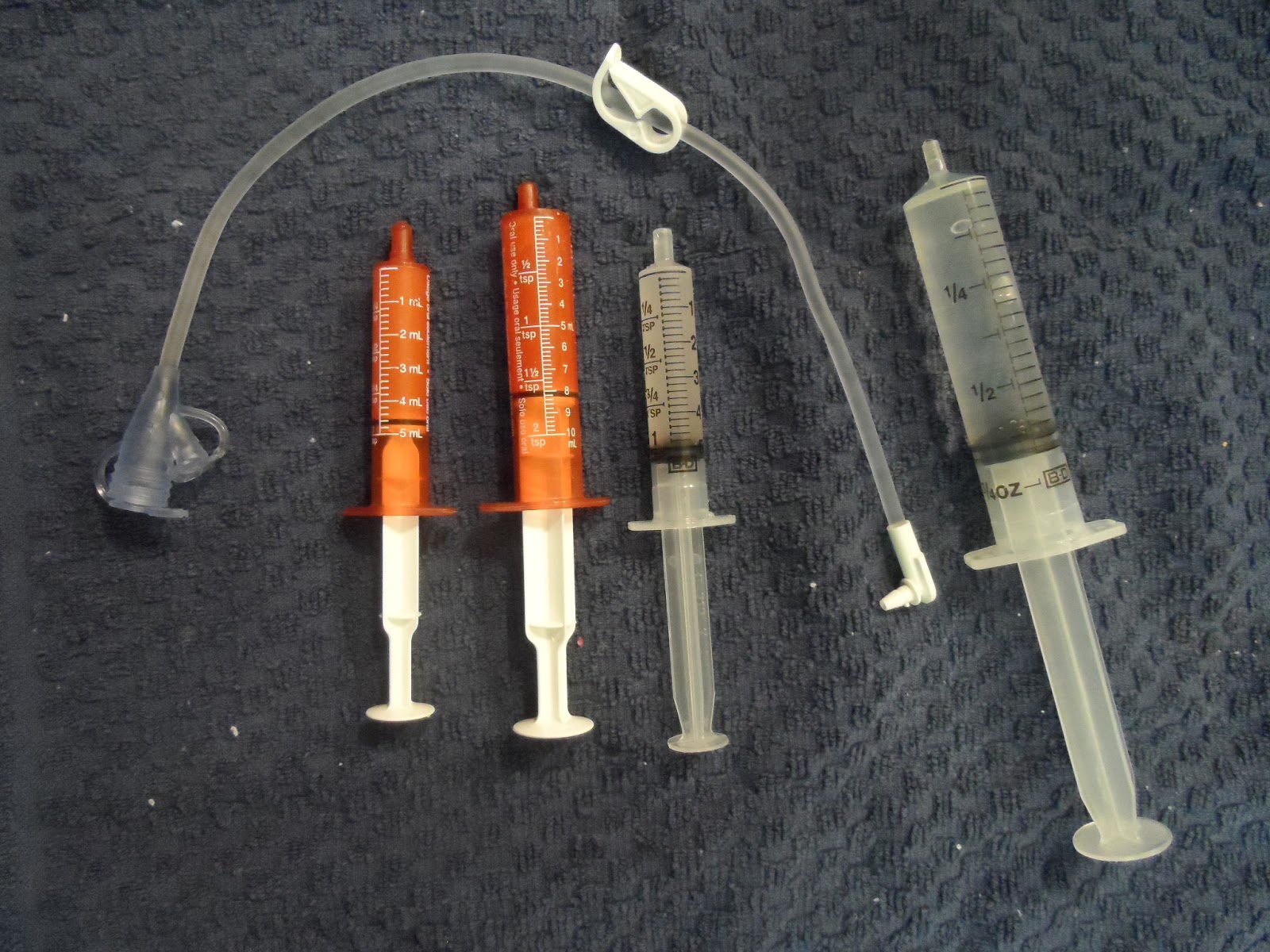
| A view of the whole tube we use to give him feedings and medicine. A close up of the white part on the right is shown in pictures above. The left part is the head of the tube which has two ports. In the middle is a clamp. In this picture the clamp is open. |
 |
| The larger port on top is for feedings and the smaller one coming off the side is for his medicines. They feed into the tube the same way, they're just different sizes for different syringes to attach. In the background you see a syringe that is full of water. The syringes that fit into his feeding tube are called a "slip-tip." Some people assume we mean a syringe that could also hold a needle (like for a shot) but these just have a little tip on the end that fits into the port. |
 |
| The slip-tip syringe fitted into the medicine port and filling the tube. We prime the tube with water prior to attaching it to his button for any feeding or medicine. Otherwise we'd be pushing a bunch of air into his belly and make him burpy or even sick. After the medicine or formula is in we flush the tube with water before detaching it from his button. |
 | |||
| Here's his nightly line up: Prilosec (to help decrease stomach acid), a daily vitamin (tablet is crushed up & mixed with water because he won't eat them yet), Captopril (helps his heart function), and the water flush. The clamp on the tube is closed to hold in the water. |
 | ||||||||
| Eli has started helping with his medicines. He'll put his finger on the plunger and help us push it in. He's half asleep in this photo. You can see how it's hooked up to his button and the medicine syringe is attached. |
Some people want to know how we keep it straight. Most of the time it's pretty easy because his meds are pretty consistent. Two of them he takes twice a day, his vitamin is everyday, and he gets half a baby aspirin every other day. We do that one on even dates only 2nd, 4th, 6th, and so on). If a month has 31 days then he will he will have his aspirin the 30th, miss the 31st, miss the 1st, then have it again on the 2nd. Otherwise it gets too confusing! I created an Excel spreadsheet with his meds, their purpose, the amount & dosage, how many times a day he gets each one, a list of "as needed" meds & their dosages (Tylenol, Dimetapp, etc), and a place to mark Zachary's daily vitamins. I printed that and cut it to fit into an 8x10 frame. We use dry erase markers each day for the date and times we give him the meds. There's room to add additional info we have for the day. For example, he's on an antibiotic right now so it's written to the side with its times given.
 |
| A look at our daily board |
 | |||
| The first picture I took of our daily board being held by our lovely model. |
That's all there is to it. When we were still in talks about going the G-tube route it seemed like it would be a lot of work and a big deal, but it isn't. We just made it part of our routine and hardly even think about it. It's so convenient to be able to give Eli his medicines and feedings. We don't have to wake him if something is due when he's sleeping. We don't have to fight to get him to take multiple meds multiple times a day. He takes some by mouth, but when he initiates it. We figure he's going to be taking medicine for the rest of his life so why make it a negative experience for him? Using the tube became so normal to us that I messed up when Zachary was on an antibiotic for the first time. He was 3 1/2 and had been sick enough to require an antibiotic. It was liquid of course and supposed to be given every 8 hours. I gave him his first dose as soon as we got it from the pharmacy which was about 4pm. Next dose at midnight, right? Well, midnight rolls around and I wake to my alarm ringing, go to the kitchen, measure it out and go to his bedside. Only after getting him to roll onto his back in his sleep did I realize he didn't have a feeding tube to put it through!!! I felt soooo stupid. It wasn't a momentary lapse of intelligence, it was an 8 hour lapse during which time I just assumed the act of giving Zachary medicine would be as easy as doing it for Eli. I didn't wake him but we just changed our schedule to be more realistic for him the next day.
I hope this answers some questions for anyone who has wondered about this. Again, the invitation is out there for you to ask anything you've wondered about Eli's condition, how we handle it, etc. Use the comment section on this blog, use Facebook, or email me at jessveale@yahoo.com. Thanks for reading and remember to cherish Every Little Beat...
No comments:
Post a Comment